Position of the museum's exhibition department. Regulations on exhibition activities of the Russian Orthodox Church. His Holiness Patriarch Kirill chaired the next meeting of the Supreme Church Council
Current page: 1 (book has 35 pages total) [available reading passage: 23 pages]
Selected lectures on faculty surgery
The doctors medical sciences, professors: Kokhanenko N. Yu., Kabanov M. Yu., Ulyanov Yu. N., Pavelets K. V.; medical candidates Sciences, Associate Professor: Ananyev N.V., Lataria E.D., Ivanov A.L., Lugovoy A.L., Shiryaev Yu.N.; medical candidates Sciences: Morgoshiya T. Sh., Protchenkov M. A., Zaitsev A. V., Galkina N. V.
Reviewers:
Dudanov I. 77. – Head of the Departments of General and Faculty Surgery of Petrozavodsk state university, corresponding member RAMS professor. Maistrenko N. A.– Head of the Department of Faculty Surgery named after. prof. S. P. Fedorov Military Medical Academy named after. S. M. Kirova, corresponding member. RAMS, professor.
Breast diseases
Anatomy and physiology of the breast
Mammary (mammary) gland (mamma) is a paired apocrine gland of epidermal origin, producing a specific secretion (milk).
Normally, a person has one pair of mammary glands. As an atavism, accessory mammary glands are found, which can be located in the anterior axillary region or on the abdomen, often only on one side; the nipple and areola may be absent. In men, the mammary gland remains in a rudimentary form throughout life, but in women, with the onset of puberty, it increases in size. The mammary glands go through several stages in their development. After birth, the mammary glands in girls and boys are practically no different from each other. During puberty, with the beginning of the functioning of the ovaries, the mammary glands begin to increase in volume, and with the onset of menstruation, their tissue undergoes monthly cyclic changes in accordance with the phases of the menstrual cycle. By the period of menopause, the glands undergo involutive changes - fatty degeneration. The mammary gland reaches its greatest development towards the end of pregnancy, although milk production (lactation) occurs already in the postpartum period.
The mammary gland is located anterior to the fascia of the pectoralis major muscle, with which it is connected by loose connective tissue, which determines its mobility. Supporting ligaments (Cooper's ligaments) pass through the entire thickness of the gland, extending from the superficial fascia, from the leaves of which the capsule of the gland itself is formed, and intertwining into the deep layers of the skin. In women, the glands are located symmetrically on both sides of the anterior surface of the chest from the III to VI ribs, reaching medially to the edge of the sternum, and laterally to the mid-axillary line. Somewhat downwards from the center of the gland, on its anterior surface there is a nipple, papilla mammae, at the top of which the main milk passages open. The nipple is surrounded by a pigmented area of skin - the areola mammae. In the area of the areola and nipple there are circular and longitudinal muscle fibers, the contraction of which tightens the nipple, which facilitates the evacuation of secretions when feeding the baby.
The mammary gland, by its type of structure, belongs to the complex alveolar-tubular glands. The gland tissue itself consists of 15–20 cone-shaped isolated lobules, which converge radially with their tips towards the nipple. The excretory ducts of each lobule are connected into a milky passage, which is directed to the nipple and ends at its apex with a small hole separate for each lobule. In the retroareolar region, the milk ducts have ampulla-shaped extensions, which during lactation serve as a kind of reservoir for milk secreted between feedings.
The blood supply to the mammary glands comes from aa. intercostales posteriores, a. thoracica interna and a. thoracica lateralis. Venous outflow from the gland tissue occurs into the basin of the superior vena cava through vessels that partly accompany the named arteries, partly go under the skin, forming a network with wide loops.
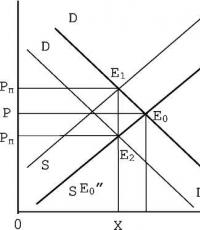
Lymphatic drainage from breast tissue occurs along several routes, which determines significant variability in the zones of lymphogenous metastasis. The following lymph nodes are regional to the mammary gland (Fig. 1).
Axillary: interpectoral lymph nodes (Rotter) and lymph nodes located along the axillary vein and its tributaries. Most of the lymph flows through these pathways (more than 90%). According to the 2002 International Union Against Cancer classification, intramammary lymph nodes are also coded as axillary.
They are divided into 3 levels.
Level I – (lower axillary): lymph nodes located lateral to the lateral border of the pectoralis minor muscle.
Level II – (middle axillary): lymph nodes located between the medial and lateral edges of the pectoralis minor muscle, as well as interpectoral lymph nodes (Rotter’s lymph nodes).
Level III – (upper axillary): lymph nodes located medial to the medial edge of the pectoralis minor muscle, including the subclavian and apical.
Internal lymph nodes of the mammary gland (on the affected side): parasternal lymph nodes located in the endothoracic fascia and intercostal spaces along the edge of the sternum.
The rest of the lymph drainage from the mammary gland can be carried out, bypassing the regional lymph nodes: along the intercostal tract; through the skin, subcutaneous and retrosternal lymphatic vessels into the lymphatic system of the opposite gland (cross path of metastasis); through the lymphatic vessels of the epigastric region and further into the lymph nodes of the coronary ligament of the liver, retroperitoneal and inguinal lymph nodes (Gerota’s path).
Rice. 1. Lymphatic vessels and regional lymph nodes of the mammary gland. 1 - paramammary lymph nodes: a - Bartels node, 6 - Sorgius node; 2 – lateral axillary nodes; 3 – central axillary lymph nodes; 4 – subscapular lymph nodes; 5 - subclavian lymph nodes; 6 - supraclavicular lymph nodes; 8 – interthoracic lymph nodes; 9 – retrosternal lymph nodes; 10 – lymphatic vessels directed to the epigastric region. (Credited from: Atlas of Oncological Operations.
Ed. B.E. Peterson. M., 1987)
The spread of tumor cells along these pathways creates the prerequisites for the occurrence of distant lymph node metastases in the corresponding groups of lymph nodes (Fig. 2).
The iron receives sensory nerves from II–V nn. intercostales. The branches of the nn also take part in the innervation of the skin covering the gland. pectorales mediales et laterales from the brachial plexus and nn. supraclaviculares from the cervical plexus. Sympathetic nerves penetrate the gland along with blood vessels.
The condition and functioning of the mammary glands throughout a woman’s life are regulated by various hormones produced by the endocrine glands (ovaries, adrenal glands, pituitary system, hypothalamus). Most of these hormones are steroidal and have the same precursor - cholesterol. Hormonal regulation is a complex mechanism of endocrine interactions that operate on the feedback principle. With the onset of puberty, the concentration of estrogen in the female body increases, which determines the growth and functional maturation of the mammary glands. The development of breast tissue and their function are regulated by female sex hormones (estrogens, progesterone), as well as human chorionic gonadotropin, prolactin. Particular importance in stimulating the development of mammary gland tissue and other female secondary sexual characteristics is given to estrogens, the production of which occurs mainly in the ovaries during the entire childbearing period. During each menstrual cycle, breast tissue undergoes cyclic changes: after ovulation, under the influence of progesterone produced by the corpus luteum, the growth of the alveoli is stimulated, and the size of the gland increases slightly. If pregnancy does not occur, then after menstruation the level of progesterone production decreases sharply, and the size of the mammary gland also decreases. After this, a new Graafian vesicle matures in the ovaries, the level of estrogen produced in the ovaries gradually increases, which leads to the next ovulation, and the cycle repeats.

Rice. 2. Pathways for lymph drainage from the mammary gland
(scheme). 1 – paramammary lymph nodes; 2 – central axillary lymph nodes; 3 - subclavian lymph nodes; 4 - supraclavicular lymph nodes; 5 – deep cervical lymph nodes; 6 – parasternal lymph nodes; 7 - cross lymphatic pathways connecting the lymphatic systems of both mammary glands; 8 – lymphatic vessels going into the abdominal cavity; 9 – superficial inguinal lymph nodes.
The level of sex hormones undergoes natural physiological fluctuations not only during each menstrual cycle, but also during pregnancy, childbirth, and breastfeeding. In the regulation of this process, the normal functioning of almost all hormonal organs, as well as systems responsible for the inactivation and excretion of hormones (kidneys, liver), is important. Clinical evidence suggests that deviations in the intensity and timing of these physiological mechanisms increase the risk of breast cancer.
Partial involution of the mammary glands with the onset of menopause is associated with the cessation of the functioning of the ovaries, which are the main producers of estrogens in women of childbearing age. However, even after the cessation of menstruation, a certain amount of estrogens is formed in a woman’s body - in the adrenal glands, as well as due to the aromatization of androgens in adipose tissue, muscles, and internal organs.
Fibroadenomatosis
Fibroadenomatosis (FAM) of the mammary glands is a very common pathology that occurs, according to different authors, in 30–60% of all women. In 1984, WHO proposed the term fibrocystic breast disease for this pathology. In the International Classification of Diseases (X), this nosological form is designated as benign mammary dysplasia. IN foreign literature The term "benign breast disease" is often used. In the domestic literature, the terms FAM, dyshormonal mammary hyperplasia, and mastopathy are usually used. In 1985, the Russian Ministry of Health proposed a convenient clinical and radiological classification of mastopathy, which is most often used today. Mastopathy, according to this classification, is divided into 2 main forms, each of which has subtypes. In particular, they distinguish:
1) diffuse mastopathy:
a) with a predominance of the glandular component (adenosis);
b) with a predominance of the fibrous component (fibrosis);
c) with a predominance of the cystic component (multiple cysts);
d) mixed form (glandular-cystic).
2) nodular mastopathy:
a) fibroadenoma;
In oncological practice, the term FAM is more often used, which will be used further. With FAM, patients usually complain of mastalgia (pain in the mammary glands), premenstrual tension syndrome (heaviness and swelling of the mammary glands during the premenstrual period), dysalgomenorrhea (painful, unsystematic periods). Palpation reveals compactions and swelling in the mammary glands; with echographic and mammographic studies - cysts and fibroadenomatous changes; morphological examination reveals hyperplasia of epithelial cells and fibroblasts in the lobular and ductal structures of the mammary glands, sclerosis and atrophy.
The problem of FAM is very relevant, since, according to surveys, at an outpatient appointment with an oncologist, up to 50% of patients are patients with this pathology. FAM as a separate nosological entity was identified at the end of the 19th century, and for several decades this disease was considered as a stage preceding the onset of breast cancer. Currently, views on FAM have undergone significant changes. In general, this pathology is not a precancer or stage of an oncological process in the mammary glands. Precancer of the mammary glands is a morphological concept; it includes ductal atypical hyperplasia of the epithelium and carcinoma in situ, lobular atypical epithelial hyperplasia and carcinoma in situ; in the presence of these changes, the risk of invasive breast cancer (BC) increases by 2.5-10 times or more. FAM is considered as one of the many risk factors for breast cancer. Precancerous changes are found in only a small proportion of women with FAM. However, the role of FAM in the development of breast cancer should not be underestimated.
There are 4 groups of evidence linking FAM with breast cancer:
1) for FAM and breast cancer – common factors risk;
2) the causes and mechanisms of development of FAM and breast cancer have common features, a key role is played by a relative or absolute excess of estrogens - long-term chronic hyperestrogenism;
3) when the mammary glands are removed due to a cancerous tumor, various morphological manifestations of FAM can often be detected in the tissues;
4) in retrospective and prospective epidemiological studies, previous FAM is more often identified in patients with breast cancer. However, the issue of the relationship between FAM and breast cancer is controversial. According to various authors, FAM can increase the risk of developing breast cancer by 1.5 times or have no effect on it at all. All women suffering from FAM cannot be considered at risk for developing breast cancer. The most significant changes are the morphological changes in the mammary gland tissue. According to epidemiological studies, in patients with FAM, with hyperproliferation of the epithelium without atypia, the risk of developing cancer increases by 2–3 times, with hyperproliferation of the epithelium with atypia – by 5–7 times. Monitoring women suffering from FAM and providing therapy for this disease is aimed at preventing breast cancer. However, the scientific and practical aspects of the problem of FAM continue to remain controversial in oncology. In addition, modern medicine simply does not have the technical capabilities to adequately monitor and treat the huge contingent of women suffering from FAM. Unfortunately, in our country, the efforts of the oncology service aimed at identifying, treating and clinically examining patients with FAM did not lead to the goal of reducing the incidence of breast cancer.
For nodular forms of FAM, sectoral resection of the mammary gland with urgent histological examination of the gross specimen is indicated. Using two semi-oval incisions in the radial direction relative to the areola, the affected sector of the gland is excised to the fascia of the pectoralis major muscle, and then the wound is sutured in layers (Fig. 3).
Depending on the results of an urgent histological examination, the operation is either completed if the process is benign, or (if cancer is detected) it is expanded to the extent of a radical operation.
Diffuse forms of FAM are subject to conservative treatment, which is aimed at regulating dysfunction of the endocrine glands, treating diseases of the female genital organs, and suppressing proliferative processes in the mammary gland.

Rice. 3. Excision of the breast sector.
(Credited from: Atlas of Oncological Operations. Ed. B.E. Peterson. M., 1987)
To relieve pain, electrophoresis with novocaine and potassium iodide is used. To reduce proliferative processes in the mammary gland in women under 40 years of age, treatment with microdoses of iodine is recommended ( water solution 0.25% potassium iodide during the intermenstrual period, 10 ml once a day after meals for 1 year). The use of microdoses of iodine is based on stimulation of the production of luteinizing hormone by the pituitary gland. This hormone normalizes the function of ovaries with a disrupted luteal phase and restores the normal cycle of changes in the mammary gland. If the function of the corpus luteum is insufficient, progesterone is used in the second half of the menstrual cycle.
Mammary cancer
Relevance of the problem and prevalence of the diseaseBreast cancer ranks first in the structure of cancer diseases in women, accounting for 19.5%, and the incidence is constantly growing. Thus, in 1980, the number of patients registered by oncology institutions Russian Federation with a newly diagnosed diagnosis per 100 thousand female population was 30.7, in 1990 - 39.6, and in 1998 already - 55.0. The maximum incidence rates of breast cancer in 1996 were registered in the Northwestern (43.2 per 100 thousand population), Central (38.6) and Far Eastern (35.4) regions of our country.
In European countries, 180,000 new cases of cancer of this localization are registered annually, and in the USA - more than 130,000. At the same time, the number of cases is increasing in each country, adding 1-2% annually. Thus, in the 21st century, if such an increase in the incidence of breast cancer continues, the threshold of 1,000,000 cases per year will be overcome.
Despite the fact that breast tumors are tumors of external localization, and the organ is easily accessible for research, stage I–II cancer is diagnosed in only 57.6% of patients, and the mortality rate in the first year from the moment of diagnosis is 12.6%. Thus, patients with advanced forms of breast cancer account for 42.4%. Analysis of the causes of neglect, conducted by the Oncological Institute named after. P. A. Herzen, showed that this is largely due to the low medical culture of the population. At the same time, 42% of patients from this contingent put off their visit to the doctor by all means, citing employment, family circumstances, an unfavorable situation at work, etc., 10.9% of patients openly stated that they were afraid to go to the doctor, 6. 5% self-medicated, which often led to rapid progression of the disease. However, in 32.5% of cases, the neglect of the tumor was entirely on the conscience of the general medical network doctors, due to their low oncological literacy and lack of oncological alertness. In 51.7% of patients, from the moment the first clinical signs of breast cancer appear until diagnosis is made, it takes from 1 to 6 months.
The geography of breast cancer distribution is also heterogeneous. The highest incidence rates were observed in women living in Hawaii, British Columbia and California. In these areas, the incidence rate is 80–90 cases per 100 thousand women. The smallest number of cases occurs in Japan, where breast cancer occurs in 12–15 cases per 100 thousand women. In Eastern Europe, 40–60 cases per 100 thousand women are detected annually. The incidence is heterogeneously represented in different social strata. Thus, according to Finnish authors, the greatest risk of developing breast cancer is observed among representatives of a high social class. In Italy, mortality from breast cancer in more developed countries northern regions country is more than 2 times higher than in southern rural areas.
Among the administrative territories of the Russian Federation, the highest incidence is observed in the Republic of North Ossetia (49.5 per 100 thousand people), St. Petersburg (49.0), Magadan region (48.2), Moscow (46.4). Thus, for residents of St. Petersburg and the North-Western region of Russia, this problem is especially relevant.
Etiology and pathogenesisThe mammary gland is an organ reproductive system women. Therefore, among the causes of cancer, dishormonal disorders caused by dysfunction of the ovaries, adrenal glands, thyroid gland, and hypothalamus are in first place. The mechanisms of dishormonal disorders leading to the development of breast cancer have not yet been fully studied. However, there is a clear connection between the incidence of breast cancer and childbearing. Thus, the indigenous residents of Central Asia, Transbaikalia and the Far North, unlike the Russians living there, do not use contraceptives, do not have abortions, give birth at a younger age, have more repeat births and breastfeed their children for a long time. The incidence of breast cancer in this category of women is the lowest in the country. The protective role of lactation against breast cancer is a decrease in estrogenic activity during this period, as well as the fact that chemical carcinogens and mutant cells are removed from the mammary gland with milk. According to American authors, a woman who gave birth for the first time at age 18 has a three times lower risk of developing breast cancer than a woman who gave birth for the first time at age 35. Early first pregnancy contributes to a sharp increase in the production of one of the three estrogens - estriol, which is a product of the metabolism of estradiol and estrone and inhibits the carcinogenic effects of the latter. On the other hand, late first birth (after 0 years of breastfeeding) leads to a sharp increase in estradiol levels, which may contribute to the development of breast cancer. With an increase in the number of births, the level of prolactin in the blood serum decreases, the excess of which can act on the mammary gland as a carcinogen.
Many patients associate the appearance of a malignant tumor in their mammary gland with various mental traumas, that is, with various stressful situations. This is easy to understand if we consider that such stress is accompanied by the release of corticoids into the blood, which have immunosuppressive properties.
Up to 25% of women suffering from breast cancer report a history of mechanical trauma to the affected gland.
Among blood relatives of sick women, breast cancer occurs 8.5 times more often than in the entire population.
Many authors indicate that the risk of breast cancer increases 3.5 times among women with a history of three or more abortions. The corpus luteum fully blossoms during pregnancy. After termination of pregnancy, it continues to function for a long time, as a result of which changes in the hormonal balance occur in the body, accompanied by a predominance of proliferation processes.
In the development of dishormonal disorders, a significant role is played by inflammatory processes in the pelvis and, first of all, inflammatory diseases of the uterine appendages, which can cause gross structural and functional disorders of the pituitary-ovarian axis.
: tutorial Team of authors
Selected lectures on faculty surgery
Selected lectures on faculty surgery
Doctors of Medical Sciences, Professors: Kokhanenko N. Yu., Kabanov M. Yu., Ulyanov Yu. N., Pavelets K. V.; medical candidates Sciences, Associate Professor: Ananyev N.V., Lataria E.D., Ivanov A.L., Lugovoy A.L., Shiryaev Yu.N.; medical candidates Sciences: Morgoshiya T. Sh., Protchenkov M. A., Zaitsev A. V., Galkina N. V.
Reviewers: Dudanov I. 77. – Head of the Departments of General and Faculty Surgery of Petrozavodsk State University, corresponding member. RAMS professor. Maistrenko N. A.– Head of the Department of Faculty Surgery named after. prof. S. P. Fedorov Military Medical Academy named after. S. M. Kirova, corresponding member. RAMS, professor.
From the book History of Medicine by E. V. Bachilo39. Development of surgery in Russia At the end of the 19th century. Abdominal surgery began to develop widely; a large number of abdominal surgeries. For example: gastroenterostomy (G. Matveev, T. Billroth), pylorotomy (J. Pean), excision of the cecum (T. Billroth),
From the book Operative Surgery author I. B. Getman7. Lasers in surgery The mechanism of action of a laser scalpel is based on the fact that the energy of a monochromatic, coherent light beam sharply increases the temperature in a corresponding limited area of the body and leads to its instant combustion and evaporation. Thermal
From the book Operative Surgery: Lecture Notes author I. B. Getman52. Concept of endoscopic surgery Endoscopic surgery is a field of surgery that allows radical operations or diagnostic procedures to be performed through pinpoint punctures of tissue or through natural physiological openings. The idea of performing visual
From the book The Newest Victories of Medicine by Hugo Glaser5. Lasers in surgery The mechanism of action of a laser scalpel is based on the fact that the energy of a monochromatic, coherent light beam sharply increases the temperature in a corresponding limited area of the body and leads to its instant combustion and evaporation. Thermal
From the book Child's Health and the Common Sense of His Relatives author Evgeny Olegovich KomarovskyAdvances in brain surgery Many thousands of years ago, mankind knew about the operation of craniotomy. During excavations of ancient graves and burials in deep layers of the earth, skulls with well-healed burr holes were and are still being found. Ancient and
From the book Code yourself to be slim author Mikhail Borisovich IngerleibPart Four SELECTED ARTICLES I prefer to find one truth, even in insignificant things, than to argue for a long time about the greatest issues without achieving any truth. Galileo Galilei A small preface The fourth part of the book combines the most
From the book History of Medicine author Pavel Efimovich ZabludovskySide effects of surgery
From the book The Many Faces of Virus author Victor Abramovich ZuevProblems of surgery Soviet surgery has achieved significant success in solving problems of heart and vascular surgery, surgery of the respiratory system, esophagus, stomach, nephrosurgery, and transplantology. To develop scientific problems in surgery during the years of Soviet power, it was created
From the book Food Corporation. The whole truth about what we eat author Mikhail GavrilovLectures with a strange title Early March morning 1954, students and teachers Faculty of Medicine University of London were quite surprised by the announcement that Professor of the Reykjavik Institute of Experimental Pathology Björn Sigurdson
From the book Doctors Who Changed the World author Kirill SukhomlinovFor reference (excerpts from a lecture by Ermakova I.V., Professor, Doctor of Biological Sciences) The situation with GM crops in the world. The first transgenic products were developed back in the late 80s. Since 1996, the total area under crops under transgenic crops has increased 50 times and in 2005 amounted to 90 million
From the book Philosophy of Health author Team of authors -- Medicine From the book Battle of Psychics. How it works? author Mikhail Viktorovich Vinogradov From the book Treatment of Children with Unconventional Methods. Practical encyclopedia. author Stanislav Mikhailovich Martynov From the book Quit Smoking! SELF-coding according to the SOS system author Vladimir Ivanovich Zvyagin From the author's bookSelected questions about the health of young children Why selected? Yes, because the selection of these materials is based on questions from parents and answers to them. It seems that the topics they touched on are of certain practical interest for our people today.
From the author's bookLectures-meditations For almost 30 years now, I have been asking every smoker who comes to me for the first time for help the same question: “Have you previously undergone treatment to quit smoking or tried to do it on your own?” Most of the time I heard an affirmative
Selected lectures on faculty surgery
Doctors of Medical Sciences, Professors: Kokhanenko N. Yu., Kabanov M. Yu., Ulyanov Yu. N., Pavelets K. V.; medical candidates Sciences, Associate Professor: Ananyev N.V., Lataria E.D., Ivanov A.L., Lugovoy A.L., Shiryaev Yu.N.; medical candidates Sciences: Morgoshiya T. Sh., Protchenkov M. A., Zaitsev A. V., Galkina N. V.
Reviewers: Dudanov I. 77. – Head of the Departments of General and Faculty Surgery of Petrozavodsk State University, corresponding member. RAMS professor. Maistrenko N. A.– Head of the Department of Faculty Surgery named after. prof. S. P. Fedorov Military Medical Academy named after. S. M. Kirova, corresponding member. RAMS, professor.
Breast diseases
Anatomy and physiology of the breast
Mammary (mammary) gland (mamma) is a paired apocrine gland of epidermal origin, producing a specific secretion (milk).
Normally, a person has one pair of mammary glands. As an atavism, accessory mammary glands are found, which can be located in the anterior axillary region or on the abdomen, often only on one side; the nipple and areola may be absent. In men, the mammary gland remains in a rudimentary form throughout life, but in women, with the onset of puberty, it increases in size. The mammary glands go through several stages in their development. After birth, the mammary glands in girls and boys are practically no different from each other. During puberty, with the beginning of the functioning of the ovaries, the mammary glands begin to increase in volume, and with the onset of menstruation, their tissue undergoes monthly cyclic changes in accordance with the phases of the menstrual cycle. By the period of menopause, the glands undergo involutive changes - fatty degeneration. The mammary gland reaches its greatest development towards the end of pregnancy, although milk production (lactation) occurs already in the postpartum period.
The mammary gland is located anterior to the fascia of the pectoralis major muscle, with which it is connected by loose connective tissue, which determines its mobility. Supporting ligaments (Cooper's ligaments) pass through the entire thickness of the gland, extending from the superficial fascia, from the leaves of which the capsule of the gland itself is formed, and intertwining into the deep layers of the skin. In women, the glands are located symmetrically on both sides of the anterior surface of the chest from the III to VI ribs, reaching medially to the edge of the sternum, and laterally to the mid-axillary line. Somewhat downwards from the center of the gland, on its anterior surface there is a nipple, papilla mammae, at the top of which the main milk passages open. The nipple is surrounded by a pigmented area of skin - the areola mammae. In the area of the areola and nipple there are circular and longitudinal muscle fibers, the contraction of which tightens the nipple, which facilitates the evacuation of secretions when feeding the baby.
The mammary gland, by its type of structure, belongs to the complex alveolar-tubular glands. The gland tissue itself consists of 15–20 cone-shaped isolated lobules, which converge radially with their tips towards the nipple. The excretory ducts of each lobule are connected into a milky passage, which is directed to the nipple and ends at its apex with a small hole separate for each lobule. In the retroareolar region, the milk ducts have ampulla-shaped extensions, which during lactation serve as a kind of reservoir for milk secreted between feedings.
The blood supply to the mammary glands comes from aa. intercostales posteriores, a. thoracica interna and a. thoracica lateralis. Venous outflow from the gland tissue occurs into the basin of the superior vena cava through vessels that partly accompany the named arteries, partly go under the skin, forming a network with wide loops.
Lymphatic drainage from breast tissue occurs along several routes, which determines significant variability in the zones of lymphogenous metastasis. The following lymph nodes are regional to the mammary gland (Fig. 1).
Axillary: interpectoral lymph nodes (Rotter) and lymph nodes located along the axillary vein and its tributaries. Most of the lymph flows through these pathways (more than 90%). According to the 2002 International Union Against Cancer classification, intramammary lymph nodes are also coded as axillary.
They are divided into 3 levels.
Level I – (lower axillary): lymph nodes located lateral to the lateral border of the pectoralis minor muscle.
Level II – (middle axillary): lymph nodes located between the medial and lateral edges of the pectoralis minor muscle, as well as interpectoral lymph nodes (Rotter’s lymph nodes).
Level III – (upper axillary): lymph nodes located medial to the medial edge of the pectoralis minor muscle, including the subclavian and apical.
Internal lymph nodes of the mammary gland (on the affected side): parasternal lymph nodes located in the endothoracic fascia and intercostal spaces along the edge of the sternum.
The rest of the lymph drainage from the mammary gland can be carried out, bypassing the regional lymph nodes: along the intercostal tract; through the skin, subcutaneous and retrosternal lymphatic vessels into the lymphatic system of the opposite gland (cross path of metastasis); through the lymphatic vessels of the epigastric region and further into the lymph nodes of the coronary ligament of the liver, retroperitoneal and inguinal lymph nodes (Gerota’s path).
Rice. 1. Lymphatic vessels and regional lymph nodes of the mammary gland. 1 - paramammary lymph nodes: a - Bartels node, 6 - Sorgius node; 2 – lateral axillary nodes; 3 – central axillary lymph nodes; 4 – subscapular lymph nodes; 5 - subclavian lymph nodes; 6 - supraclavicular lymph nodes; 8 – interthoracic lymph nodes; 9 – retrosternal lymph nodes; 10 – lymphatic vessels directed to the epigastric region. (Credited from: Atlas of Oncological Operations. Ed. B.E. Peterson. M., 1987)
The spread of tumor cells along these pathways creates the prerequisites for the occurrence of distant lymph node metastases in the corresponding groups of lymph nodes (Fig. 2).
The iron receives sensory nerves from II–V nn. intercostales. The branches of the nn also take part in the innervation of the skin covering the gland. pectorales mediales et laterales from the brachial plexus and nn. supraclaviculares from the cervical plexus. Sympathetic nerves penetrate the gland along with blood vessels.
Doctors of Medical Sciences, Professors: Kokhanenko N. Yu., Kabanov M. Yu., Ulyanov Yu. N., Pavelets K. V.; medical candidates Sciences, Associate Professor: Ananyev N.V., Lataria E.D., Ivanov A.L., Lugovoy A.L., Shiryaev Yu.N.; medical candidates Sciences: Morgoshiya T. Sh., Protchenkov M. A., Zaitsev A. V., Galkina N. V.
Reviewers: Dudanov I. 77. – Head of the Departments of General and Faculty Surgery of Petrozavodsk State University, Corresponding Member. RAMS professor. Maistrenko N. A.– Head of the Department of Faculty Surgery named after. prof. S. P. Fedorov Military Medical Academy named after. S. M. Kirova, corresponding member. RAMS, professor.
Breast diseases Anatomy and physiology of the breast
Mammary (mammary) gland (mamma) is a paired apocrine gland of epidermal origin, producing a specific secretion (milk).
Normally, a person has one pair of mammary glands. As an atavism, accessory mammary glands are found, which can be located in the anterior axillary region or on the abdomen, often only on one side; the nipple and areola may be absent. In men, the mammary gland remains in a rudimentary form throughout life, but in women, with the onset of puberty, it increases in size. The mammary glands go through several stages in their development. After birth, the mammary glands in girls and boys are practically no different from each other. During puberty, with the beginning of the functioning of the ovaries, the mammary glands begin to increase in volume, and with the onset of menstruation, their tissue undergoes monthly cyclic changes in accordance with the phases of the menstrual cycle. By the period of menopause, the glands undergo involutive changes - fatty degeneration. The mammary gland reaches its greatest development towards the end of pregnancy, although milk production (lactation) occurs already in the postpartum period.
The mammary gland is located anterior to the fascia of the pectoralis major muscle, with which it is connected by loose connective tissue, which determines its mobility. Supporting ligaments (Cooper's ligaments) pass through the entire thickness of the gland, extending from the superficial fascia, from the leaves of which the capsule of the gland itself is formed, and intertwining into the deep layers of the skin. In women, the glands are located symmetrically on both sides of the anterior surface of the chest from the III to VI ribs, reaching medially to the edge of the sternum, and laterally to the mid-axillary line. Somewhat downwards from the center of the gland, on its anterior surface there is a nipple, papilla mammae, at the top of which the main milk passages open. The nipple is surrounded by a pigmented area of skin - the areola mammae. In the area of the areola and nipple there are circular and longitudinal muscle fibers, the contraction of which tightens the nipple, which facilitates the evacuation of secretions when feeding the baby.
The mammary gland, by its type of structure, belongs to the complex alveolar-tubular glands. The gland tissue itself consists of 15–20 cone-shaped isolated lobules, which converge radially with their tips towards the nipple. The excretory ducts of each lobule are connected into a milky passage, which is directed to the nipple and ends at its apex with a small hole separate for each lobule. In the retroareolar region, the milk ducts have ampulla-shaped extensions, which during lactation serve as a kind of reservoir for milk secreted between feedings.
The blood supply to the mammary glands comes from aa. intercostales posteriores, a. thoracica interna and a. thoracica lateralis. Venous outflow from the gland tissue occurs into the basin of the superior vena cava through vessels that partly accompany the named arteries, partly go under the skin, forming a network with wide loops.
Lymphatic drainage from breast tissue occurs along several routes, which determines significant variability in the zones of lymphogenous metastasis. The following lymph nodes are regional to the mammary gland (Fig. 1).
Axillary: interpectoral lymph nodes (Rotter) and lymph nodes located along the axillary vein and its tributaries. Most of the lymph flows through these pathways (more than 90%). According to the 2002 International Union Against Cancer classification, intramammary lymph nodes are also coded as axillary.
They are divided into 3 levels.
Level I – (lower axillary): lymph nodes located lateral to the lateral border of the pectoralis minor muscle.
Level II – (middle axillary): lymph nodes located between the medial and lateral edges of the pectoralis minor muscle, as well as interpectoral lymph nodes (Rotter’s lymph nodes).
Level III – (upper axillary): lymph nodes located medial to the medial edge of the pectoralis minor muscle, including the subclavian and apical.
Internal lymph nodes of the mammary gland (on the affected side): parasternal lymph nodes located in the endothoracic fascia and intercostal spaces along the edge of the sternum.
The rest of the lymphatic drainage from the mammary gland can be carried out, bypassing the regional lymph nodes: along the intercostal tract; through the skin, subcutaneous and retrosternal lymphatic vessels into the lymphatic system of the opposite gland (cross path of metastasis); through the lymphatic vessels of the epigastric region and further into the lymph nodes of the coronary ligament of the liver, retroperitoneal and inguinal lymph nodes (Gerota’s path).

Rice. 1. Lymphatic vessels and regional lymph nodes of the mammary gland. 1 – paramammary lymph nodes: a – Bartels node, 6 – Sorgius node; 2 – lateral axillary nodes; 3 – central axillary lymph nodes; 4 – subscapular lymph nodes; 5 – subclavian lymph nodes; 6 – supraclavicular lymph nodes; 8 – interthoracic lymph nodes; 9 – retrosternal lymph nodes; 10 – lymphatic vessels directed to the epigastric region. (Credited from: Atlas of Oncological Operations.Ed. B.E. Peterson. M., 1987)
The spread of tumor cells along these pathways creates the prerequisites for the occurrence of distant lymph node metastases in the corresponding groups of lymph nodes (Fig. 2). The iron receives sensory nerves from II–V nn. intercostales. The branches of the nn also take part in the innervation of the skin covering the gland. pectorales mediales et laterales from the brachial plexus and nn. supraclaviculares from the cervical plexus. Sympathetic nerves penetrate the gland along with blood vessels.
The condition and functioning of the mammary glands throughout a woman’s life are regulated by various hormones produced by the endocrine glands (ovaries, adrenal glands, pituitary system, hypothalamus). Most of these hormones are steroidal and have the same precursor - cholesterol. Hormonal regulation is a complex mechanism of endocrine interactions that operate on the feedback principle. With the onset of puberty, the concentration of estrogen in the female body increases, which determines the growth and functional maturation of the mammary glands. The development of breast tissue and their function are regulated by female sex hormones (estrogens, progesterone), as well as human chorionic gonadotropin, prolactin. Particular importance in stimulating the development of mammary gland tissue and other female secondary sexual characteristics is given to estrogens, the production of which occurs mainly in the ovaries during the entire childbearing period. During each menstrual cycle, breast tissue undergoes cyclic changes: after ovulation, under the influence of progesterone produced by the corpus luteum, the growth of the alveoli is stimulated, and the size of the gland increases slightly. If pregnancy does not occur, then after menstruation the level of progesterone production decreases sharply, and the size of the mammary gland also decreases. After this, a new Graafian vesicle matures in the ovaries, the level of estrogen produced in the ovaries gradually increases, which leads to the next ovulation, and the cycle repeats.

Rice. 2. Pathways for lymph drainage from the mammary gland(scheme). 1 – paramammary lymph nodes; 2 – central axillary lymph nodes; 3 – subclavian lymph nodes; 4 – supraclavicular lymph nodes; 5 – deep cervical lymph nodes; 6 – parasternal lymph nodes; 7 – cross lymphatic pathways connecting the lymphatic systems of both mammary glands; 8 – lymphatic vessels going into the abdominal cavity; 9 – superficial inguinal lymph nodes. (Credited from: Atlas of Oncological Operations. Ed. B.E. Peterson. M., 1987)
The level of sex hormones undergoes natural physiological fluctuations not only during each menstrual cycle, but also during pregnancy, childbirth, and breastfeeding. In the regulation of this process, the normal functioning of almost all hormonal organs, as well as systems responsible for the inactivation and excretion of hormones (kidneys, liver), is important. Clinical evidence suggests that deviations in the intensity and timing of these physiological mechanisms increase the risk of breast cancer. Partial involution of the mammary glands with the onset of menopause is associated with the cessation of the functioning of the ovaries, which are the main producers of estrogens in women of childbearing age. However, even after the cessation of menstruation, a certain amount of estrogens is formed in a woman’s body - in the adrenal glands, as well as due to the aromatization of androgens in adipose tissue, muscles, and internal organs.
Selected lectures on faculty surgery
Doctors of Medical Sciences, Professors: Kokhanenko N. Yu., Kabanov M. Yu., Ulyanov Yu. N., Pavelets K. V.; medical candidates Sciences, Associate Professor: Ananyev N.V., Lataria E.D., Ivanov A.L., Lugovoy A.L., Shiryaev Yu.N.; medical candidates Sciences: Morgoshiya T. Sh., Protchenkov M. A., Zaitsev A. V., Galkina N. V.
Reviewers: Dudanov I. 77. – Head of the Departments of General and Faculty Surgery of Petrozavodsk State University, corresponding member. RAMS professor. Maistrenko N. A.– Head of the Department of Faculty Surgery named after. prof. S. P. Fedorov Military Medical Academy named after. S. M. Kirova, corresponding member. RAMS, professor.
Breast diseases
Anatomy and physiology of the breast
Mammary (mammary) gland (mamma) is a paired apocrine gland of epidermal origin, producing a specific secretion (milk).
Normally, a person has one pair of mammary glands. As an atavism, accessory mammary glands are found, which can be located in the anterior axillary region or on the abdomen, often only on one side; the nipple and areola may be absent. In men, the mammary gland remains in a rudimentary form throughout life, but in women, with the onset of puberty, it increases in size. The mammary glands go through several stages in their development. After birth, the mammary glands in girls and boys are practically no different from each other. During puberty, with the beginning of the functioning of the ovaries, the mammary glands begin to increase in volume, and with the onset of menstruation, their tissue undergoes monthly cyclic changes in accordance with the phases of the menstrual cycle. By the period of menopause, the glands undergo involutive changes - fatty degeneration. The mammary gland reaches its greatest development towards the end of pregnancy, although milk production (lactation) occurs already in the postpartum period.
The mammary gland is located anterior to the fascia of the pectoralis major muscle, with which it is connected by loose connective tissue, which determines its mobility. Supporting ligaments (Cooper's ligaments) pass through the entire thickness of the gland, extending from the superficial fascia, from the leaves of which the capsule of the gland itself is formed, and intertwining into the deep layers of the skin. In women, the glands are located symmetrically on both sides of the anterior surface of the chest from the III to VI ribs, reaching medially to the edge of the sternum, and laterally to the mid-axillary line. Somewhat downwards from the center of the gland, on its anterior surface there is a nipple, papilla mammae, at the top of which the main milk passages open. The nipple is surrounded by a pigmented area of skin - the areola mammae. In the area of the areola and nipple there are circular and longitudinal muscle fibers, the contraction of which tightens the nipple, which facilitates the evacuation of secretions when feeding the baby.
The mammary gland, by its type of structure, belongs to the complex alveolar-tubular glands. The gland tissue itself consists of 15–20 cone-shaped isolated lobules, which converge radially with their tips towards the nipple. The excretory ducts of each lobule are connected into a milky passage, which is directed to the nipple and ends at its apex with a small hole separate for each lobule. In the retroareolar region, the milk ducts have ampulla-shaped extensions, which during lactation serve as a kind of reservoir for milk secreted between feedings.
The blood supply to the mammary glands comes from aa. intercostales posteriores, a. thoracica interna and a. thoracica lateralis. Venous outflow from the gland tissue occurs into the basin of the superior vena cava through vessels that partly accompany the named arteries, partly go under the skin, forming a network with wide loops.
Lymphatic drainage from breast tissue occurs along several routes, which determines significant variability in the zones of lymphogenous metastasis. The following lymph nodes are regional to the mammary gland (Fig. 1).
Axillary: interpectoral lymph nodes (Rotter) and lymph nodes located along the axillary vein and its tributaries. Most of the lymph flows through these pathways (more than 90%). According to the 2002 International Union Against Cancer classification, intramammary lymph nodes are also coded as axillary.